ARFID vs Sensory Sensitivity: What We’re Still Getting Wrong About Restrictive Eating
Is it ARFID or sensory sensitivity? Learn the nervous system science behind restrictive eating in ADHD and autism, and why traditional approaches often fail.
ARFID, Sensory Sensitivity, or Something Deeper?
There is a question that comes up repeatedly in neurodivergent spaces:
“Is this ARFID… or is it just sensory sensitivity?”
It sounds like a diagnostic question.
But what it actually reveals is something more fundamental:
We are still trying to explain a nervous system pattern using behavioural language.
And that mismatch is where most interventions begin to fail.
Understanding Avoidant/Restrictive Food Intake Disorder
Clinically, ARFID is defined by:
• persistent restriction or avoidance of food
• driven by sensory sensitivity, fear, or lack of interest
• leading to nutritional, social, or functional impact
What it is not defined by:
• body size
• weight alone
• “picky eating”
This matters, because many individuals who struggle with restrictive eating, especially those with ADHD and autism, are often overlooked if they do not fit the stereotypical presentation.
This is not about preference.
It is about processing.
Food is a full sensory experience:
• texture
• smell
• visual variation
• temperature
• oral-motor demand
• internal body response (interoception)
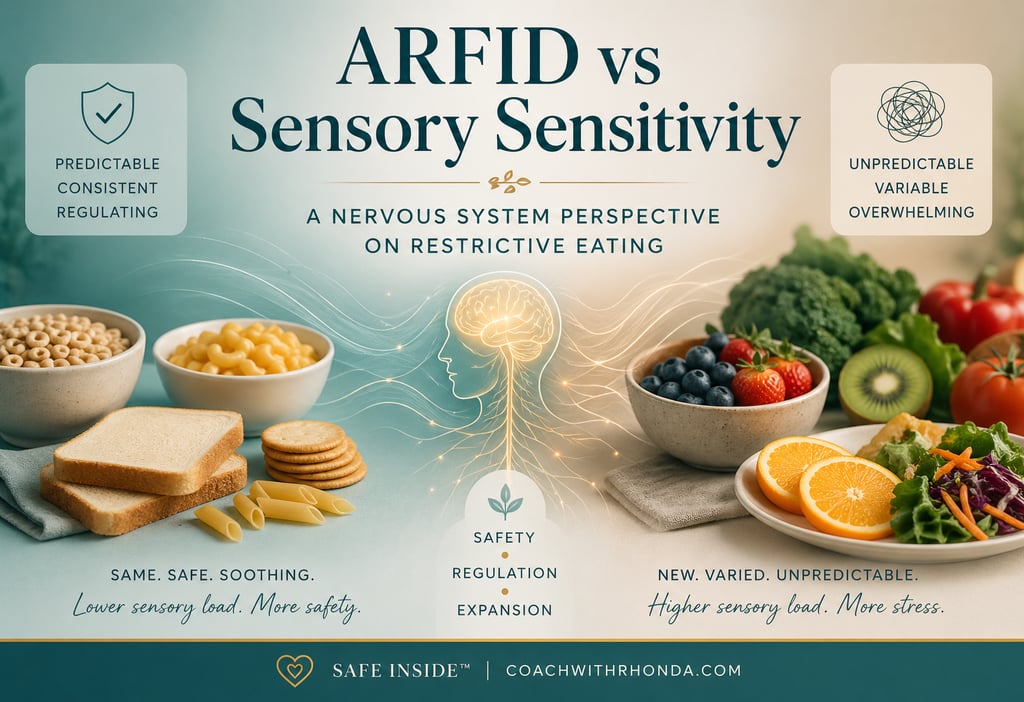
For a sensitive nervous system, especially in neurodivergence, variability is not neutral.
It is unpredictable.
And unpredictability is one of the fastest ways to trigger a stress response.
The Mechanism Most People Miss
Why “Unhealthy” Foods Often Feel Safer
Highly processed foods are often:
• consistent
• predictable
• uniform in texture and taste
They reduce:
• sensory load
• cognitive effort
• uncertainty
In other words, they are regulating.
By contrast, foods often labeled as “healthy,” such as fruits and vegetables, are:
• inconsistent
• variable in taste and texture
• harder to predict
From a nutritional perspective, they are beneficial.
From a nervous system perspective, they can be high-demand inputs.
Why Traditional Approaches Often Fail
The dominant model is simple:
Increase exposure → increase tolerance
But this assumes the nervous system experiences exposure as neutral.
In many cases, it does not.
Instead, it is experienced as:
• pressure
• overwhelm
• loss of control
Which reinforces avoidance.
Not because someone is unwilling, but because the system is protecting itself.
A Nervous System–Informed Approach
When we shift the lens, the strategy changes.
Instead of asking:
“How do we get someone to eat more foods?”
We ask:
“How do we reduce threat in the eating experience?”
Because when threat decreases:
• capacity increases
• tolerance expands
• flexibility becomes possible
What Actually Works
A more effective model includes:
1. Stabilization Before Change
Do not remove safe foods prematurely.
2. Nutrition Within Existing Patterns
Improve intake using current foods before expanding variety.
3. Sensory Bridging
Introduce small, controlled variations rather than entirely new foods.
4. Exposure Without Pressure
Interaction with food comes before consumption.
5. Texture Matching
New foods must align with existing sensory preferences.
6. Predictability Over Variety
Repetition builds safety. Safety builds capacity.
7. Regulation First
A dysregulated nervous system cannot expand.
Reframing Restrictive Eating
This is not:
• lack of discipline
• refusal
• defiance
It is:
• a nervous system prioritizing safety
• a reliance on predictability
• a response to sensory overload
The behaviour is not the problem.
It is the current solution.
Whether it is labeled ARFID or sensory sensitivity, the path forward remains the same:
Reduce threat.
Increase safety.
Expand capacity.
When we stop trying to override the system and begin working with it, change becomes not only possible, but sustainable.
Final Thought
© 2026 Coaching with Rhonda. All rights reserved.
Rhonda Tournay is a trauma-informed coach and educator specializing in nervous system regulation, neurodivergence, and emotional health — helping individuals, families, and professionals find safety and resilience through the Safe Inside™ Protocol.